At Mineralys, we are advancing the clinical development of lorundrostat for people with aldosterone-driven hypertension and beyond.
Lorundrostat, an investigational drug, is a novel, oral, highly selective, once-daily aldosterone synthase inhibitor (ASI).1
How it Works
Lorundrostat targets aldosterone-driven hypertension by inhibiting the enzyme that catalyzes the final steps of aldosterone synthesis. Our goal is to decrease levels of aldosterone by selectively inhibiting aldosterone synthesis without affecting cortisol synthesis. Lorundrostat has 374-fold selectivity for inhibiting aldosterone synthesis over cortisol synthesis.1
Treatment of Hypertension with Lorundrostat
In a phase 2 clinical trial, lorundrostat was effective in reducing blood pressure in people with uncontrolled hypertension taking at least 2 medications, including those on 3 or more medications (treatment-resistant hypertension), and lorundrostat was well tolerated.1
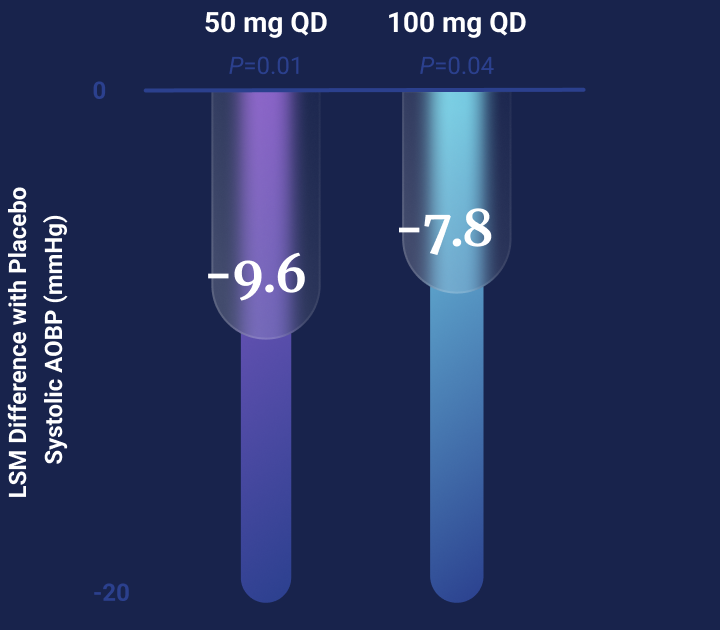
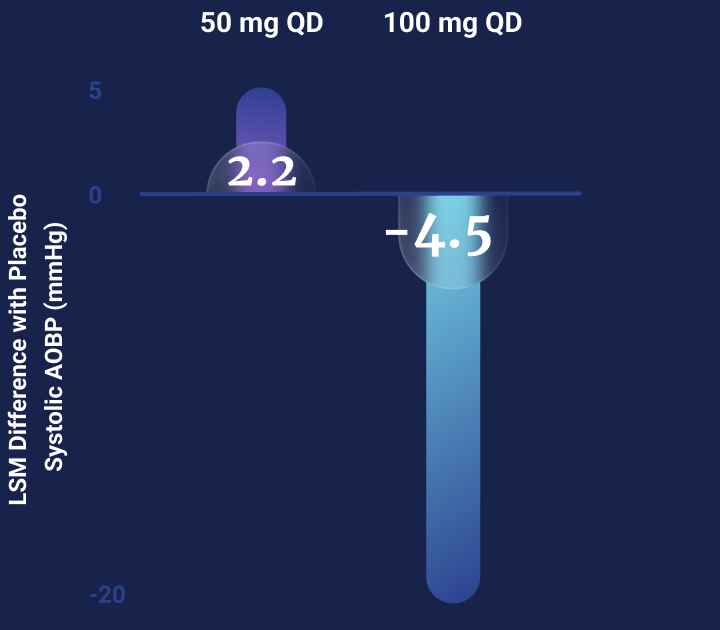
Lorundrostat at doses of 50 mg and 100 mg once-daily reduced systolic BP significantly more than placebo1
Primary Endpoint of TARGET-HTN
Primary Endpoint of TARGET-HTN
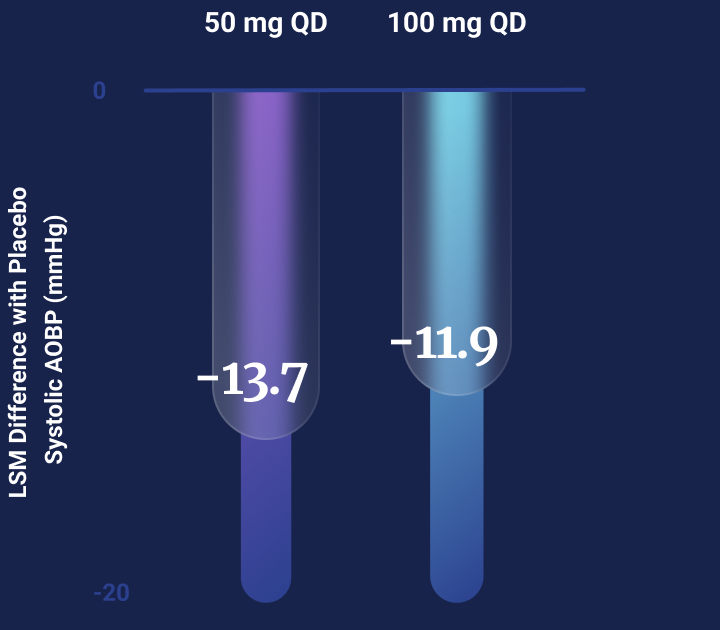
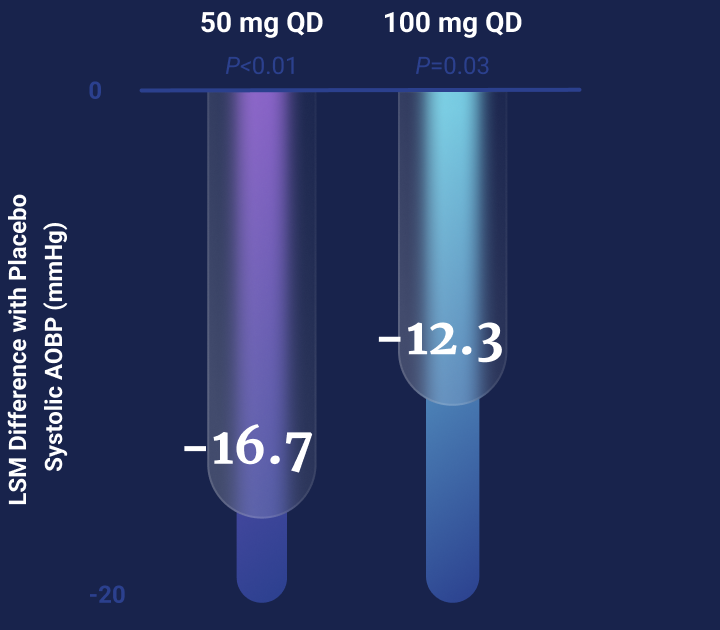
People with obesity had an enhanced response in blood pressure reduction to lorundrostat1
Placebo-Adjusted Improvement in Systolic BP by BMI
Placebo-Adjusted Improvement in Systolic BP by BMI
Lorundrostat was well tolerated across the dose range tested1
The adverse event profile was as expected for an ASI with modest changes in sodium and potassium levels observed. Only one clinically significant event was observed, worsening hyponatremia in a participant on the 100-mg once-daily dose of lorundrostat. No meaningful effect on serum cortisol levels was observed.
Ongoing clinical trials are evaluating the efficacy and safety of lorundrostat in people with uncontrolled hypertension, including treatment-resistant hypertension, and people with hypertension and chronic kidney disease.
Aldosterone is a steroid hormone that regulates blood pressure and blood volume.
It is part of the renin-angiotensin-aldosterone system (RAAS, i.e., RAAS-dependent).
Aldosterone is an independent predictor of organ damage and cardio-renal-metabolic syndrome (CRMS) events.2
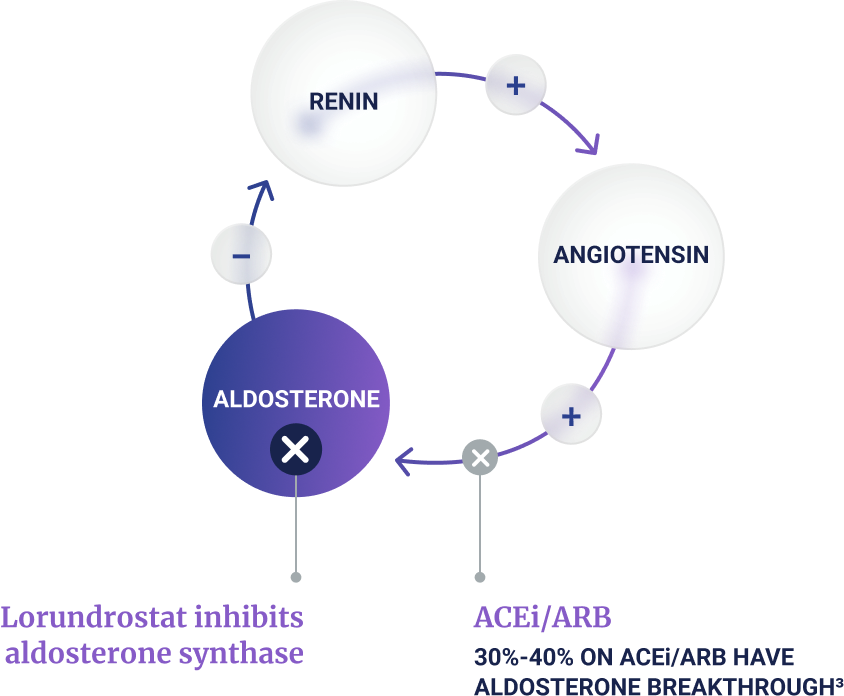
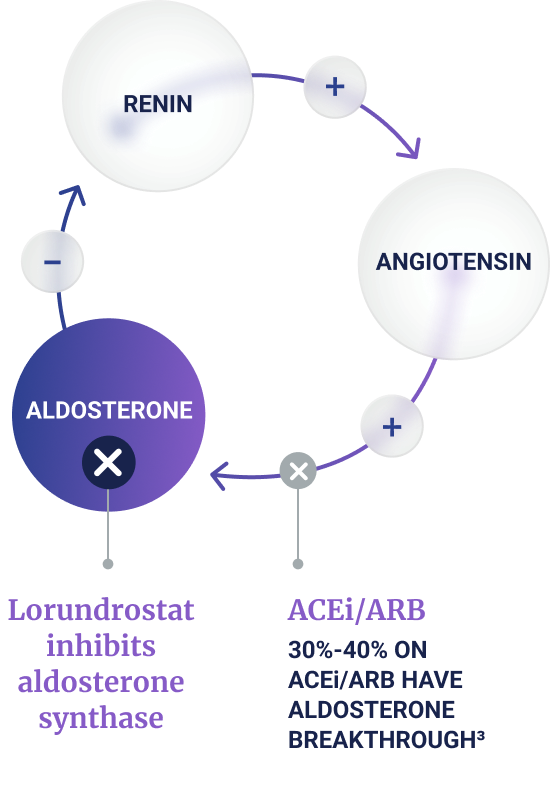
Regulation of aldosterone occurs through RAAS-dependent and RAAS-independent pathways
RAAS-Dependent Axis
Negative-feedback between aldosterone and renin maintains appropriate aldosterone levels
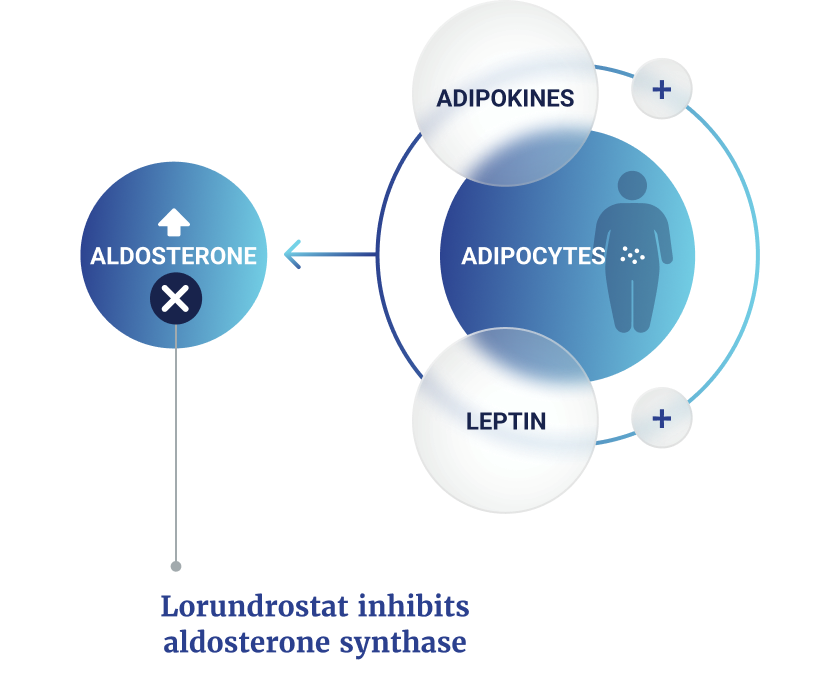
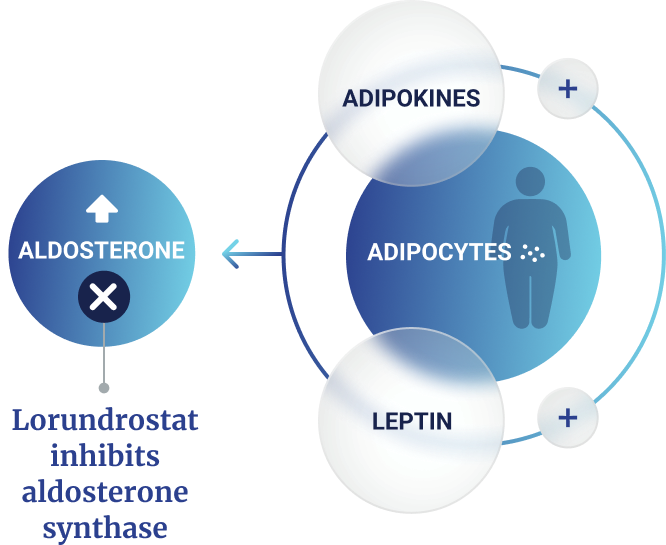
RAAS-Independent Axis
Positive-feedback between visceral adipocytes and the adrenal cortex drives dysregulated aldosterone
of people with hypertension have dysregulated aldosterone4
How it Works
Aldosterone works by binding to the mineralocorticoid receptor (MR) within cells of the kidney and other organs.5 In the classic MR pathway, aldosterone promotes sodium and water reabsorption and potassium excretion, which drives blood volume and BP.5 In addition to MR-mediated effects, aldosterone also signals through non-MR mediated pathways, such as G protein-coupled receptors.6
Dysregulated Aldosterone Due to Obesity Is a Driver of Uncontrolled
Hypertension, Including Treatment-Resistant Hypertension
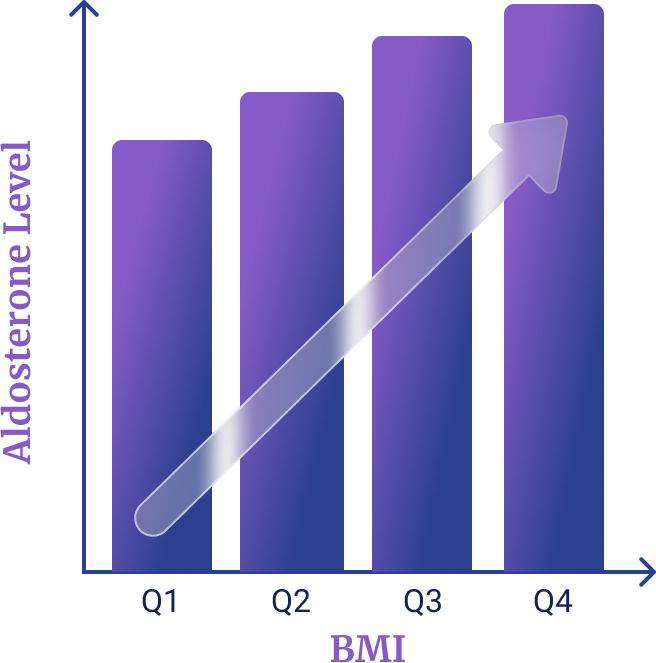
Aldosterone levels correlate significantly with BMI
In patients with treatment-resistant hypertension, 24-h urinary aldosterone (24-h UAldo µ/g) levels were significantly increased across BMI quartiles (p<0.0001)7:
BMI kg/m2
Mean 24-h UAldo µ/g
Quartile 1 (Q1) <28.1
9.2
Quartile 2 (Q2) ≥28.1 and <32.1
11.0
Quartile 3 (Q3) ≥32.1 and <36.6
12.9
Quartile 4 (Q4) ≥36.6
13.8
The link between obesity and dysregulated aldosterone occurs in both RAAS-dependent and RAAS-independent pathways.8
Obesity-related dysregulated aldosterone represents a unique endotype for hypertension.
Visceral adipocytes (belly fat cells) release adipokines that lead to the overproduction of aldosterone (dysregulated aldosterone), resulting in a wide range of complications, including uncontrolled hypertension and organ damage seen in cardio-renal-metabolic syndrome.9-12 Dysregulated aldosterone has a negative impact on the heart, kidneys, and metabolic system.13
Although treatments are available to block the effects of aldosterone through the MR, their use can result in increased levels of aldosterone14-16
Dysregulated aldosterone may lead to inflammation and fibrosis that damages the kidney and cardiovascular system.13
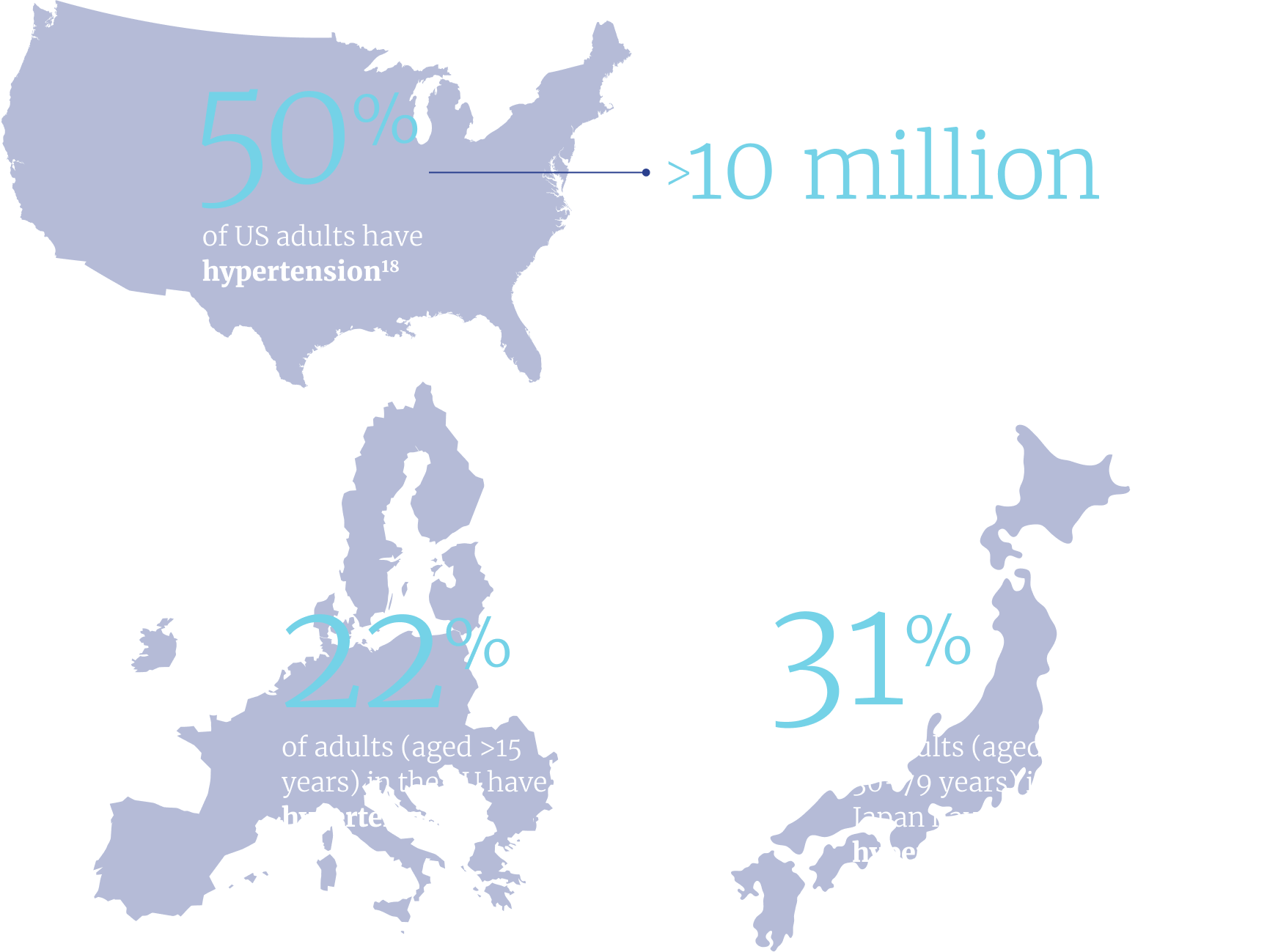
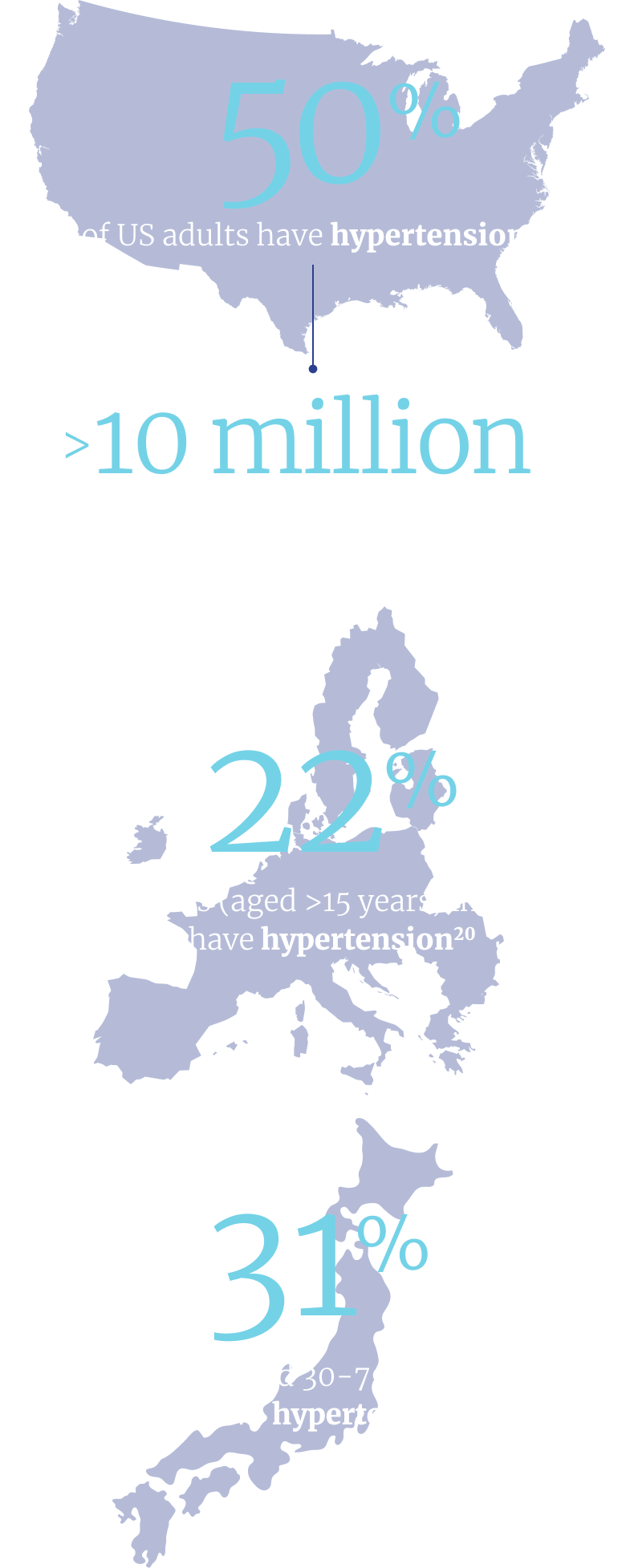
High blood pressure (hypertension) affects 1 in 3 adults worldwide and about half of adults in the US.17, 18
Despite many treatment options, over 70% of people with high blood pressure in the US have uncontrolled hypertension.22
This is because their current treatment is not reducing their blood pressure to an acceptable level.
of people with hypertension have dysregulated aldosterone.4
Despite many treatment options, over 70% of people with high blood pressure in the US have uncontrolled hypertension.22
This is because their current treatment is not reducing their blood pressure to an acceptable level.
of people with hypertension have dysregulated aldosterone.4
In general, people with treatment-resistant hypertension are those who are above blood pressure goals despite treatment with 3 or more antihypertensives, including a diuretic.23, 24
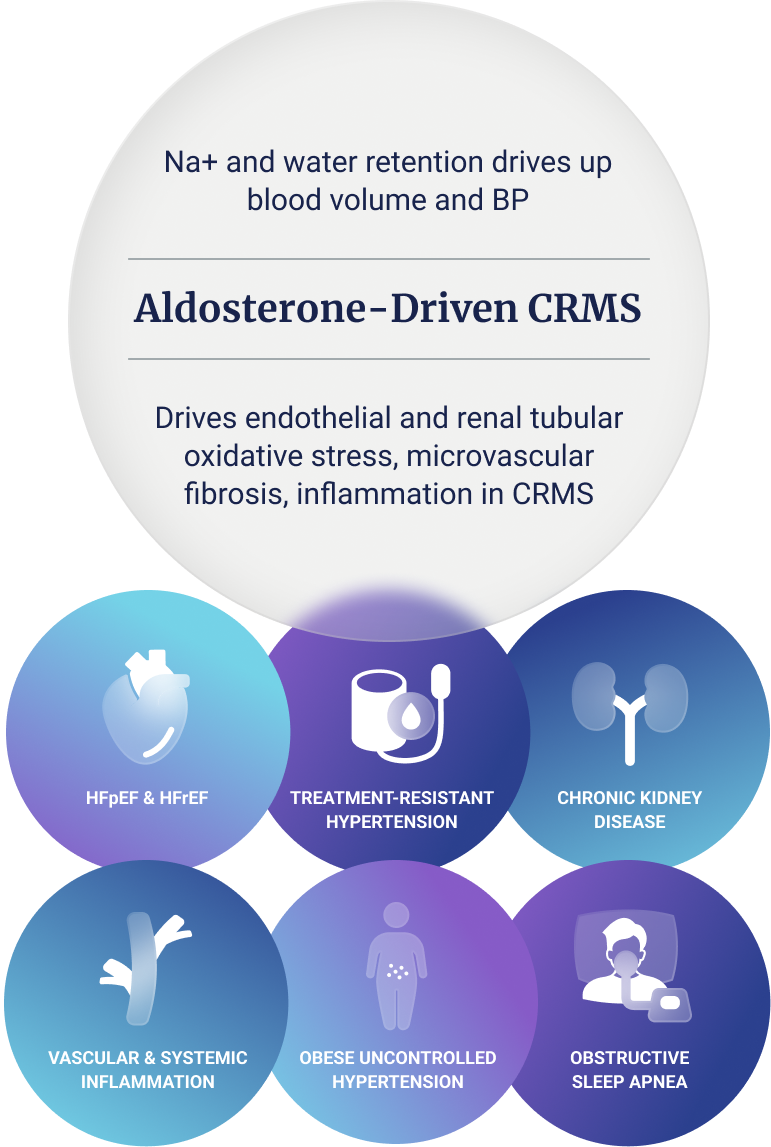
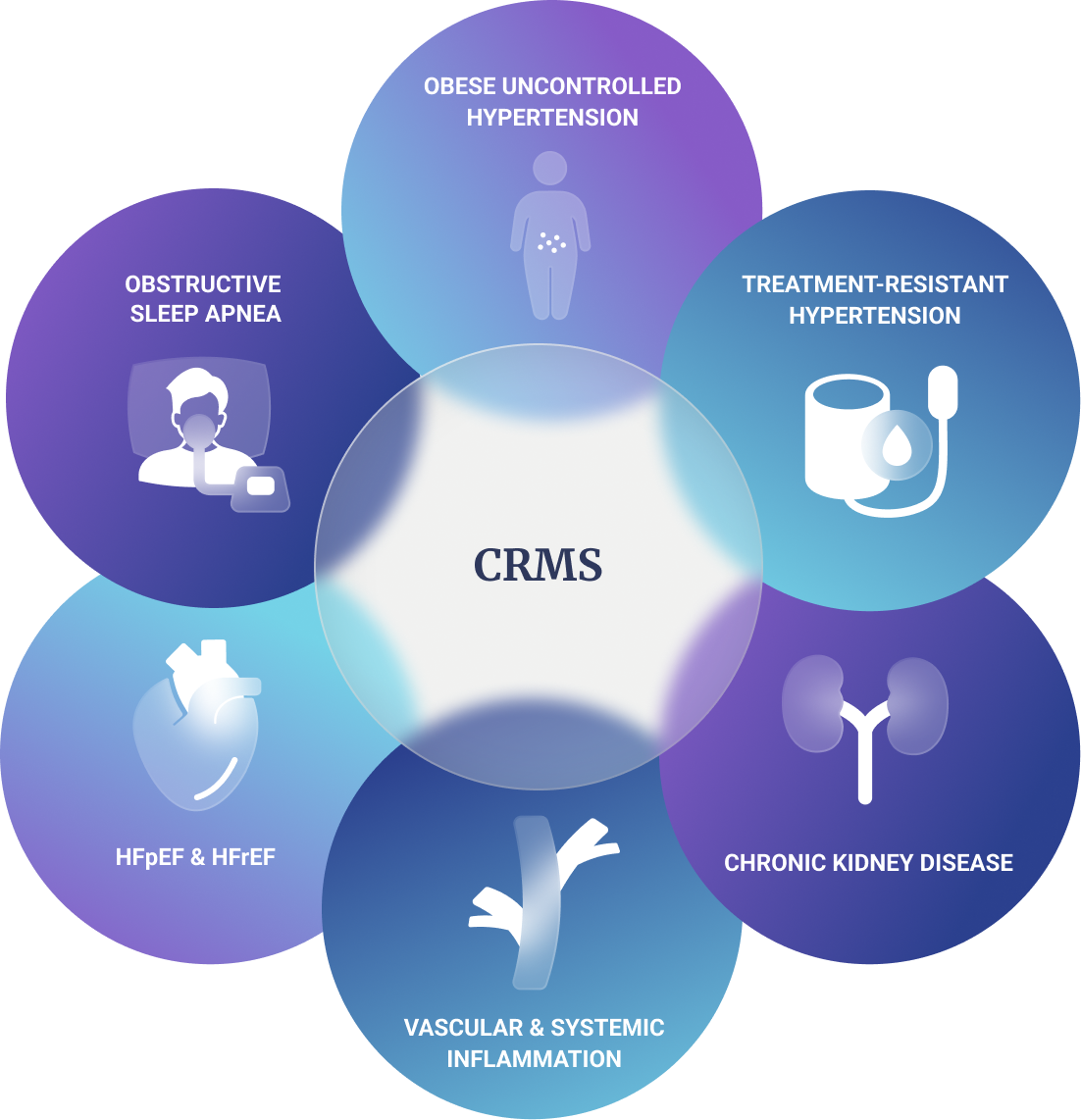
Cardio-Renal-Metabolic Syndrome
Hypertension and other CRMS diseases are major contributors to premature morbidity and mortality and are linked to dysregulated aldosterone.2,25-28
The high prevalence of hypertension and CRMS is a public health emergency.25
Dysregulated aldosterone is a key driver of uncontrolled hypertension, including treatment-resistant hypertension, and other CRMS diseases.2, 26
Uncontrolled hypertension increases the risk for other CRMS diseases such as heart failure and kidney disease.27
Dysregulated Aldosterone
The current empiric treatment strategy for people with uncontrolled hypertension, including treatment-resistant hypertension, is to add additional antihypertensive treatments.23, 24
The right treatment for the right patient
A targeted approach that identifies the right treatment for each person with uncontrolled hypertension, including treatment-resistant hypertension, is needed.
Given that elevated blood pressure is associated with an increased risk of CRMS morbidity, including cardiovascular events, stroke, and heart failure,28 a treatment approach targeting inhibition of aldosterone synthesis could potentially improve rates of blood pressure control in people with dysregulated aldosterone and reduce the risk for CRMS events.
References: 1. Laffin LJ, et al. JAMA. 2023;330(12):1140-1150. 2. Buglioni A, et al. Hypertension. 2015;65(1):45-53. 3. Bomback AS, Toto R. Am J Hypertens. 2009;22(10):1032-1040. 4. Brown JM, et al. Ann Intern Med. 2020;173(1):10-20. 5. Cannavo A, et al. Oxid Med Cell Longev. 2018:2018:1204598. 6. Briet B, Schiffrin EL. J Vasc Res. 2013;50(2):89-99. 7. Dudenbostel T, et al. Hypertension. 2016;68(4):995-1003. 8. Hall JE, et al. Nat Rev Nephrol. 2019;15(6):367-385. 9. Huby AC, et al. Hypertension. 2016;67(5):1020-1028. 10. Huby AC, et al. Circulation. 2015;132(22):2134-2145. 11. Ehrhart-Bornstein M, et al. Endocr Res. 2004;30(4):865-870. 12. De Haro Moraes C, et al. J Hum Hypertens. 2013;27(4):225-230. 13. Otsuka H, et al. Int J Mol Sci. 2023;24(6):5370. 14. Sawathiparnich P, et al. J Clin Endocrinol Metab. 2002;87:448-452. 15. Karns AD, et al. J Clin Hypertens (Greenwich). 2013;15: 186-192. 16. Calhoun DA, et al. Circulation. 2011;124:1945-1955. 17. World Health Organization. Global report on hypertension: the race against a silent killer. 2023. Available at: https://www.who.int/teams/noncommunicable-diseases/hypertension-report (Accessed May 2024). 18. Stierman B, et al. National Health and Nutrition Examination Survey 2017–March 2020 prepandemic data files—Development of files and prevalence estimates for selected health outcomes. National Health Statistics Reports; no 158. Hyattsville, MD: National Center for Health Statistics. 2021. DOI: https://dx.doi.org/10. 15620/cdc:106273. 19. Carey RM, et al. Hypertension. 2019;73(2):424-431. 20. Eurostat. Available at: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20210929-1 (Accessed September 2024). 21. World Health Organization. Hypertension Japan 2023 country profile. Available at: https://www.who.int/publications/m/item/hypertension-jpn-2023-country-profile. Accessed July 2024. 22. Centers for Disease Control and Prevention (CDC). May 12, 2023. Available at: https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html (Accessed May 2024). 23. Whelton PK, et al. Hypertension. 2018;71(6):1269-1324. 24. Mancia G, et al. J Hypertens. 2023;41(12):1874-2071. 25. Ndumele CE, et al. Circulation. 2023;148:1606-1635. 26. Acelajado MC, et al. Circ Res. 2019;124(7):1061-1070. 27. Burnier M, Damianaki A. Circ Res. 2023;132(8):1050-1063. 28. Williams B, et al. Eur Heart J. 2018;39(33):3021-3104.